Technology Imperatives To Manage The Ebola Outbreak
The Ebola outbreak serves as a portrait of the fact that the health systems of the globe must be radically interconnected in order to ensure that global outbreaks like this have a chance of being contained. We are not in the 19th century where the massive migrations of populations took place using slow-moving transport and thus where the incubation periods of most diseases would have in all likelihood passed before a person approached a border.
Today I can be infected by a disease, and within hours be on a plane that crosses the world. Traditional public health precautions of quarantining the sick will not necessarily be effective. And so we must think though a better manner of managing what is fast becoming a continental pandemic and could easily become a global pandemic.

The picture above is from the emergency room entrance at Mt. Sinai Hospital on the corner of 100th street and Madison Ave. in Manhattan.
That the disease is out of control just now is documented by the current (October 15th) World Health Organization report on the roadmap to respond to the outbreak (http://apps.who.int/iris/bitstream/10665/136508/1/roadmapsitrep15Oct2014.pdf?ua=1) which states:
“It is clear however that the situation in Guinea, Liberia and Sierra Leone is deteriorating, with widespread and persistent transmission.”

The United Nations has set up its first ever UN emergency health mission, the UN Mission for Ebola Emergency Response (UNMEER). In a press release from the UN today: “It is the position of the Security Council that the response of the international community to the Ebola outbreak has failed to date to adequately address the magnitude of the outbreak and its effects.”
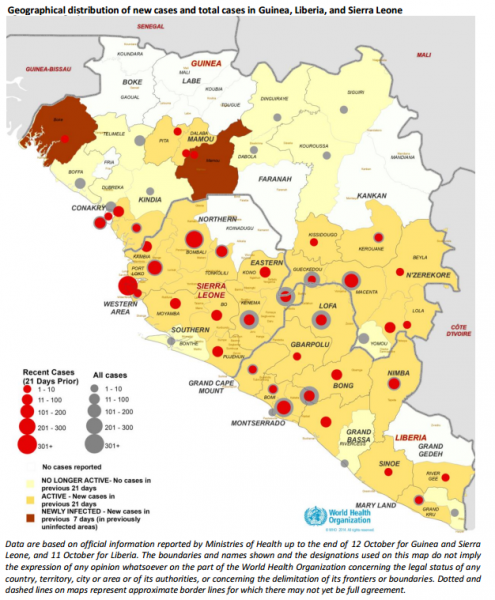
The map above is from the World Health Organization report cited above.
As of October 12, 2014, there have been 8,973 cases identified, of which 31% have occurred in the last 21 days, and of those cases there have been 4,484 deaths. To date there have been 427 cases of healthcare worker infection which is 4.8% of the total. The tone of the document from whence these statistics is derived is that in all likelihood these numbers are underreported (Source: http://apps.who.int/iris/bitstream/10665/136508/1/roadmapsitrep15Oct2014.pdf?ua=1).
So what has this to do with healthcare technology, and how can technology be brought to bear on the problem? Let’s look at the five pillars of the recommended strategy by the World Health Organization and map it to the technology imperatives that must underpin execution of the recommendations implicit or explicit in the strategy.
Case Management
At the lowest level, in order to manage a case of Ebola, isolated hospital beds are needed. Though the global community is building permanent and temporary hospitals at a fast clip, the technology needs to do so logistically are great, and yet most of these hospitals are being put up without an overall structure of program or project management being in place. Furthermore, there is a paucity of healthcare partners across the globe that can help manage this problem. Here, given the intensity of the contagion and the propensity of healthcare workers to be at significant risk, deploying remote ICU care so as to allow experts from around the world to function as clinical support would be ideal, but the tradition-bound response does not even begin to understand that this is not only a possibility but a real means to close some of the care gap that is occurring.
Case Confirmation
Minimally, in order to manage cases, good diagnostics must be allowed. In order to do this, sufficient lab capacity must be set up in order to do these tests. Even this primitive need has been hard to fulfill utilizing traditional mechanisms of transporting fully functional labs, such as the Russians have contributed on site. At present across 13 functioning labs capable of testing for Ebola, there is only a capacity to test 970 samples per day. This will not be sufficient if the outbreaks continue to grow. Here is a great place where modern infrastructures of cloud-based lab work benches deployed to more primitive work benches could facilitate the rollout, because eliminating all of the software technology from the equation of setting up a lab will make the creation of labs a simpler task.
Surveillance
The job of doing surveillance of populations at borders, within infected communities, and within the circle of those who have been in contact with victims of the disease is taking place, once again in a very traditional manner. Here is an opportunity to do remote monitoring. Give or lend to each person who must be monitored a wearable device that can measure temperature and perhaps other signs of Ebola. Ensure that they have an ability to send the resulting data to the surveillance collection point at least once a day, and by the use of normative public health powers make it a crime, where the consequences for breaking public safety law is a quarantine. The person being surveilled must link their data to the system once per day. This technology exists and can be deployed even in a third-world country, assuming there is mobile phone service. Many telehealth vendors would jump at the opportunity to run such a program. If we do this, we will vastly reduce the cost of surveillance and also potentially, if it comes to that, reduce the number of people who must be quarantined.
Safe And Dignified Burials
Tracking the dead and their belongings that might be infected is a daunting problem. Technology for managing the workflows, and metrics here would be of great use.
Social Mobilization


Millions of health workers must be trained how to manage Ebola patients. They must learn how to robe and disrobe from infection guarding suits. They must be taught the standards of care in treating Ebola and they must do so yesterday. The globe does not know where the outbreak will migrate to and thus all healthcare systems must be prepared to receive and treat Ebola patients. By all accounts the two US healthcare workers who are infected both become infected due to a lack of understanding exactly how they should have robed and disrobed. This is because they were not trained explicitly in how to do this, and this is because the global best practice for these practices has not been propagated.
The public must be informed of what their symptoms would look like if they had Ebola. They must be reassured that their own personal risk, if they are in any but the epicenter countries is low. They must be educated to be vigilant of others at risk. They must be taught when it is safe to interact with another person and when to shun them.
The only way to do these activities at the global scale we need is to ensure that technology is in place to:
1. Create the core content including protocol posters, scripts etc.
2. Translate the information into the appropriate localized content in terms of language and cultural style.
3. Propagate digital information to the community using traditional techniques as well as digital ones.